
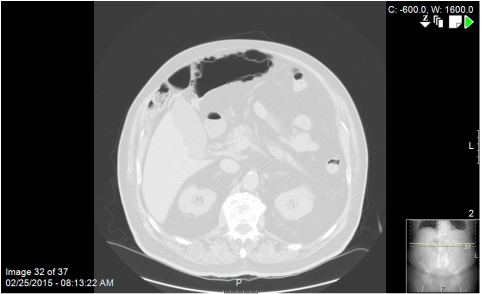
This was an older guy who presented with mild, vague upper abdominal symptoms and the above CT scan. What you should note is the air-density structure located anterior and to the left of the liver that, believe it or not, is a long redundant loop of sigmoid colon that had meandered behind a laxly fixated cecum, up the right paracolic space and behind a band of omentum above the transverse colon. The pneumatosis is obvious on the above lung windows.
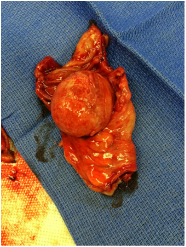
Although the guy had a relatively benign abdominal exam, I took him to the OR for laparoscopic exploration based on CT findings. His sigmoid colon snaked behind his floppy cecum and twisted like licorice as the decompressed proximal and distal limbs curved around the hepatic flexure and came to a cul de sac behind the transverse mesocolon. It took a little work identifying the ends and reducing the dilated loop but I was ultimately able to get the entire redundant sigmoid into the wound. The dilated terminus of the loop had obvious, visible pneumatosis in the muscular wall, as if someone had inserted bubble wrap just under the serosa. It was very weird to palpate. Strangely, the bowel looked entirely viable. No ischemic change. Nothing to suggest vascular compromise. Somehow, though, despite the chronic volvulus, he had been able to have bowel movements and avoid a complete colonic obstruction. I ended up performing a sigmoid resection to eliminate some of the redundancy and prevent future occurrences. He did well. When I first saw him I was fairly unimpressed; soft, non tender belly. But the radiologist talked me into it.
Although the guy had a relatively benign abdominal exam, I took him to the OR for laparoscopic exploration based on CT findings. His sigmoid colon snaked behind his floppy cecum and twisted like licorice as the decompressed proximal and distal limbs curved around the hepatic flexure and came to a cul de sac behind the transverse mesocolon. It took a little work identifying the ends and reducing the dilated loop but I was ultimately able to get the entire redundant sigmoid into the wound. The dilated terminus of the loop had obvious, visible pneumatosis in the muscular wall, as if someone had inserted bubble wrap just under the serosa. It was very weird to palpate. Strangely, the bowel looked entirely viable. No ischemic change. Nothing to suggest vascular compromise. Somehow, though, despite the chronic volvulus, he had been able to have bowel movements and avoid a complete colonic obstruction. I ended up performing a sigmoid resection to eliminate some of the redundancy and prevent future occurrences. He did well. When I first saw him I was fairly unimpressed; soft, non tender belly. But the radiologist talked me into it.

 RSS Feed
RSS Feed